



Federal health security is often discussed in broad terms, but in practice it comes down to a simple question: are medical systems prepared to function when conditions are difficult and resources are limited? For large federal agencies operating in remote and demanding environments, medical readiness is not optional. It directly affects safety and the ability to respond responsibly during emergencies.
U.S. Customs and Border Protection (CBP) is one such environment. Personnel work long hours in extreme heat, remote terrain, and unpredictable conditions. Medical emergencies may involve employees, contractors, or individuals in custody, often far from immediate hospital access. In these situations, outcomes depend on preparation and clear medical oversight.
That reality shapes the work of Alexander Eastman. A trauma surgeon and emergency medical services physician based in Dallas, Eastman has spent more than two decades working in settings where medical decisions must be made quickly and under imperfect conditions. He has also served as a sworn law-enforcement officer, an experience that informs his understanding of operational environments and the practical limits of medical response. His background in trauma care, EMS, and public safety medicine prepared him for leadership roles focused on health protection and emergency readiness at scale.
Understanding Federal Health Security in CBP Operations
Within CBP, federal health security is about whether medical systems can hold up under real operating conditions. That means making sure people have access to care when they need it, that medical decisions are properly guided in custody environments, and that teams are prepared for emergencies that may unfold far from hospitals or advanced facilities.
Much of CBP’s work happens in places where medical support is not close at hand. Long distances, harsh weather, and limited access to resources all raise the stakes when something goes wrong. In those settings, outcomes depend less on ideal equipment and more on whether the system itself is prepared, whether expectations are clear, decisions are consistent, and medical leadership is present when it matters.
Seen this way, federal health security has little to do with enforcement or policy. Its purpose is to ensure that care remains ethical, timely, and reliable even when conditions are difficult. The goal is not perfection, but stability: medical systems that continue to function when circumstances are far from controlled.
Why Emergency Preparedness Matters at the Federal Level
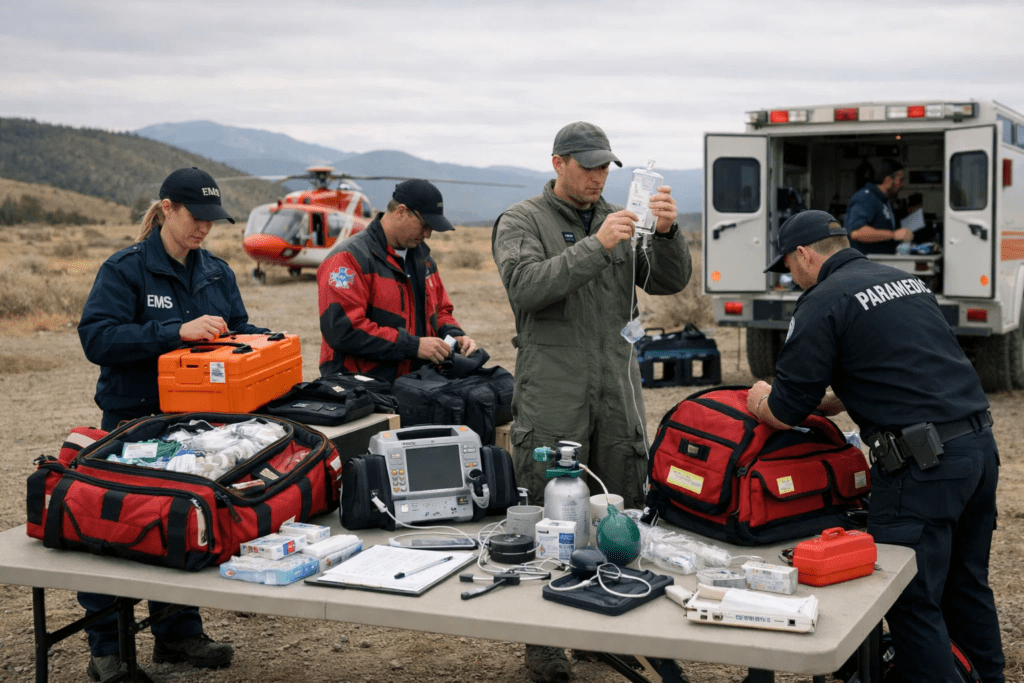
Medical staff prepared for out door emergency situation
Preparedness, in practical terms, is about whether medical systems can function when conditions are strained. It requires clear guidance for decision-making, people who are trained to work under pressure, and systems that continue to operate when information is incomplete or access is limited. Weak points tend to appear during handoffs, in remote locations, or when situations evolve faster than plans anticipate.
Eastman’s approach treats preparedness as ongoing work rather than a fixed state. It involves constant adjustment informed by training based on real events, reviewing how systems perform during stress, and refining processes before failures occur again. When medical leadership is involved early, responses tend to be more consistent, safer for those involved, and better matched to the realities faced by personnel in the field.
Dr. Alexander Eastman’s Medical Leadership Role within CBP
Within U.S. Customs and Border Protection, Alexander Eastman serves in a medical leadership capacity. His authority is limited to healthcare oversight. He does not set policy, direct enforcement activity, or influence operational decisions unrelated to health and medical care.
His responsibilities focus on ensuring that medical standards are applied consistently across the organization. This includes clinical oversight, guidance related to healthcare delivery in custody settings, and medical readiness during emergencies. The role exists to provide clear medical authority within a complex federal structure, so that health-related decisions are grounded in established medical practice rather than ad hoc judgment.
In this position, Eastman functions as a medical steward. His responsibility is to support ethical, reliable healthcare delivery and to ensure that medical systems within CBP operate within defined standards, regardless of operational pressures or situational constraints.
Applying Frontline Medical Experience to National Preparedness
Eastman’s federal work is shaped by experience gained outside Washington. His background in trauma care, emergency medical services, and public safety medicine in Dallas informs how he approaches preparedness at the national level.
Frontline work exposes where systems succeed and where they fail. It shows how quickly conditions change, how often information is incomplete, and how early decisions shape outcomes. That experience carries into federal planning by grounding preparedness efforts in what actually happens during emergencies, rather than what is assumed to happen.
Eastman’s contribution is based on translating lessons learned at the local level into systems that can function across a national organization, without relying on ideal conditions or perfect information.
How Medical Leadership Changed the System
Healthcare systems evolution and medical governance in large organizations
The most significant impact of Alexander Eastman’s leadership within CBP has been structural rather than individual. His role helped move medical decision-making from being situational and fragmented toward being more clearly defined and consistently applied across the organization.
Before that shift, medical guidance could vary depending on location, circumstance, or who happened to be involved at the moment. Eastman’s work emphasized clear medical authority, shared standards, and alignment between medical judgment and operational realities. The goal was not to create new layers of response, but to reduce uncertainty about how health decisions should be made when time and information are limited.
This approach changes how the system behaves. Medical oversight becomes part of how operations are planned and executed, rather than something consulted after problems arise. Over time, that consistency reduces reliance on improvisation and helps medical decisions hold up even when conditions are unpredictable.
From Individual Leadership to Institutional Change
System change only matters if it lasts beyond one person. Eastman’s contribution lies in helping embed medical leadership into the structure of federal operations rather than tying it to individual presence or ad-hoc influence.
When medical authority is clearly defined, it creates continuity. Standards remain in place even as personnel rotate. Expectations are clearer across teams. Decisions rely less on personal judgment and more on shared medical guidance that has already been established.
At the federal level, this matters. Large organizations cannot depend on informal processes or individual experience alone. Institutional change happens when leadership results in systems that function consistently, regardless of who is on duty or where operations are taking place. Eastman’s work reflects that shift from individual expertise to durable medical governance.
Conclusion: Leadership That Reshapes Systems
The purpose of medical leadership in federal agencies is not visibility or rapid response. It is stability. When leadership helps systems behave predictably under pressure, it reshapes how care is delivered long after individual decisions fade from view.
Through his role within CBP, Alexander Eastman’s impact is best measured not by isolated outcomes, but by how medical oversight became more clearly integrated into the organization itself. That kind of leadership does not seek attention. It strengthens the system so that, when it is tested, it holds.
That is how federal health security evolves not through individual acts, but through leadership that changes how decisions are made, every day.
{kind=link}